




Epidemiological analysis and patterns of disease amongst patients hospitalized with dengue infection across different hospitals in India
- Part 1 -
Dr. Laishram Ranbir *
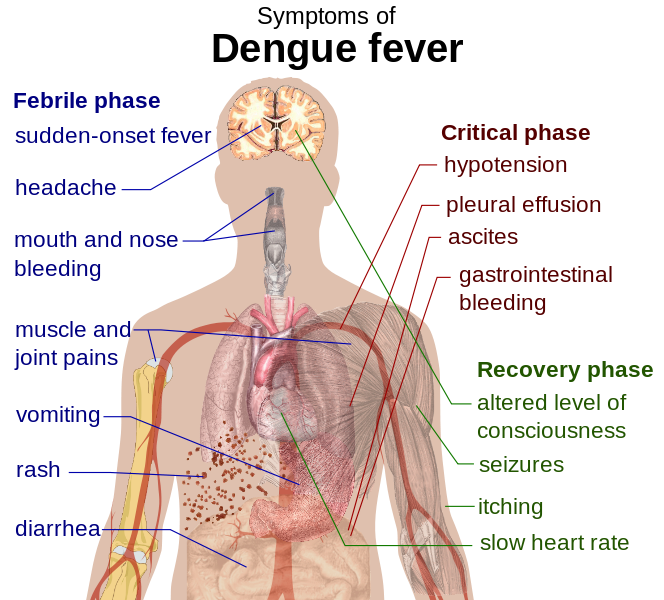
Main symptoms of dengue fever :: Pix - Wikipedia/Mikael Häggström
B.K. Tyagi.1, S. Karthigai Selvi 1, C. Vidya 1, T. Mariappan 1, P. Philip Samuel 1, R. Paramasivan 1, Mukul Gaba 2, N.K. Arora 2, S. Vivek Adhish 3, Deoki Nandan 3, Donald S. Shepard 4, Yara Halasa 4, Harish K. Pemde 5, Anurag Tomar 6, Poovazhagi Varadarajan 7, Pawan Kumar 8, Ashok Mishra 9, V.K. Srivastava 10, Koushik Vyas 11, Ranbir L. Singh 12, Bhadresh R.Vyas 13, Pallavi Shelke 14
1 Centre for Research in Medical Entomology (ICMR), 4-Sarojini Street, Chinna Chokkikulam, Madurai 625002, TN, India (Email: [email protected])
2 National Institute of Health & Family Welfare, Munirka, New Delhi
3 INCLEN Trust International, Okhla Industrial New Delhi
4 Brandeis University, 415 South Street, MS 035, Waltham, MA, USA
5 Lady Harding Medical College, New Delhi
6 NIMS Medical College, Rajasthan
7 Madras Medical College (Institute of Child Health), Tamil Nadu
8 Kasturba Medical College, Karnataka
9 G.R. Medical College, MP
10 IIMS R, UP
11 SCB Medical College, Odisha
12 RIMS, Manipur
13 M.P.Shah Medical College, Gujarat
14 LTM Medical College & General Hospital, Maharashtra
Correspondence to
Dr.B.K.Tyagi
Centre for Research in Medical Entomology (ICMR),
# 4, Sarojini Street, ChinnaChokkikulam,
Madurai-625 002, Tamilnadu, India.
Tel: + 91 452 2520565;
Fax:+ 91 452530660.
Email:[email protected]
Background and objectives: Dengue is an infectious tropical disease which has been a serious public health problem in India. The main objectives are to understand the dengue infection in the population across different region of India over six years (2006-2011) and to assess the clinical manifestations and laboratory features of patients hospitalized with dengue fever across the country.
Methods: India was divided into five regions, from each region two states with high and low incidence of dengue was selected and from each of these ten selected states, one medical college hospital was selected. The study reference year was from 2006-2011. A systematic random sampling of 1450 (From each site 50 cases of dengue every year if the cases are less than 50 all cases will be included) data set was collected from all the sites. A structured questionnaire was formulated and the data was collected including the socio demographic profile, details of hospitalisation, clinical and laboratory details. Subsequently the data was statistically analysed using SPSS version 16 and discussed.
Results: The southern region contributed around 41.12% of hospitalized cases. Of the total 1450 hospitalized cases admitted during 2006-2011, about 1219 (84.07%), 143(9.86%) and 88 (6.07%) had provisional discharge diagnosis of DF, DHF and DSS. According to WHO classification there were about 567 (39.10%) dengue suspectsand 883 (60.90%) probable dengue. The common symptoms seen for 1450 cases were fever (99.17%), vomiting (87.05%), generalized body pain (79.33), headache (74.51%), abdominal pain(61.80), liver enlargement (59.30%), myalgia (57.38%), Arthralgia (47.88%), pleural effusion (42.29%), spleen palpable (37.27%), shock (30.49%), facial flushing (26.95%), retro-orbital pain (26.94%), pedal edema (24.32%), Petechiae (22.89%), Malena (20.83%), haematemesis (16.63%) and Severe bleeding (10.62%).
Geriatric population was low in hospitalized case but registered with high mortality rate of 14.29% next to which comes the Infants (0-1 year) contributes to 8.6%. The morbidity is high among males but the mortality rate is high in the females contributing to 5.11% when compared to that of males which was 3.8%. The seasonal trend of dengue denoted a gradual increase from June with a peak in October.
Interpretation & Conclusion: Dengue being referred as a pediatric disease is now having a greater shift towards the adult population contributing to high mortality rate among the geriatric population.
Keywords
Dengue, India, clinical presentation, hospitalization, laboratory, mortality, region, diagnosis
Dengue, with its two deadly manifestations, i.e., Dengue Haemorrhagic Fever (DHF) and Dengue Shock Syndrome (DSS), has emerged into one of the major emerging infectious diseases in the world in terms of morbidity, mortality and economic burden1-3.The infection is by now viewed as a global epidemic with recorded prevalence in more than 120 countries4. During the last 200 years, spread of the disease has increased, reaching endemic proportions during the last three decades4. Worldwide, an estimated 2.5 billion people ( over 40% of the world's population)are at risk of infection with more than 50 million new infections being projected annually, and between 250,000 and 500000 cases of dengue hemorrhagic fever (DHF) that must be hospitalized and 20,00025,000 deaths, mainly in children5.The case-fatality rate for DHF ranges by country and most fatal cases are among children and young adults. Amongst the WHO SEARO countries except DPR Korea all the other countries including India are endemic for dengue6. In the last 50 years, incidence has increased 30-fold with increasing geographic expansion to new countries and, in the present decade, from urban to rural settings7
Dengue is a serious public health problem in India8-11. Till 2009, the World Health Organization has categorized India in Category B (micro level), along with Bangladesh and Maldives where cyclical epidemics are becoming more frequent, multiple virus serotypes circulating and expanding geographically within countries. However, in 2010, WHO revisited its categorization and grouped India in Category A (macro level) countries, grouped with Indonesia, Myanmar, Sri Lanka, Thailand and Timor-Leste where dengue is a major public health problem, leading cause of hospitalization and death among children, hyperendemic in urban setting now spreading to rural areas, and circulating in multiple serotypes 12
Although dengue infection has been endemic in India since the nineteenth century, dengue hemorrhagic fever (DHF) was first reported in 1963 from Calcutta city13. Since then several outbreaks of dengue fever have been reported from many states in India from time to time with a major epidemic of dengue hemorrhagic fever14-15. Major outbreaks have occurred in north India16.As on 31stDecember 2012, a total of 49576 cases and 247 deaths were reported from 33 States/UTs which is the highest in India in last two decades. Maximum cases were reported from Tamil Nadu (12264) followed by west Bengal (6456), Kerala (4172), Karnataka (3924) and Pondicherry (3506).
The case fatality rate (deaths per 100 Cases) due todengue was 3.3 % in 1996. Though it declined thereafter but consistently had been above 1.0% till 2007 and then it started declining. During last two decades from 1991 to 2012, out of 35 states/ UTs, except Lakshadweep, all the 34 states have reported Dengue cases . Dengue cases have not been reported from Arunachal Pradesh and Daman and Diu till 2011 but has recently recorded dengue cases in 2012 with 0.6% of CFR at Arunachal Pradesh.
Dengue has been an urban disease but now has spread to rural India as well due to water storage practices and large-scale development activities in rural areas, which increasing the dengue burden in the country17-22.
Unprecedented growth in population, unplanned urbanization and migration of population from rural to urban areas with lack of proper sanitation facilities are important factors resulting in increased burden of dengue in recent times23.In addition, increased distribution and densities of vector mosquitoes due to man-made, ecological and lifestyle changes along with water supply mismanagement, gaps in public health infrastructure and poor infrastructure in the states to monitor mosquito breeding were amongst the main reasons for increasing dengue cases.
India has a sentinel surveillance system which depends on selected hospitals and laboratories out of all possible hospitals/laboratories in the surveillance area for generating dengue surveillance data. This Sentinel surveillance may detect the proportion of resistance and useful for understanding the characteristics within the laboratory sentinel surveillance network. However, it is not possible to calculate the disease incidence rate as a whole. Additionally, the results of this surveillance system are not representative of the entire population owing to presence of sampling biases. In addition, there is lack of uniformity in performing the standardized laboratory based screening test between the health care providers and the test prescribed under IDSP. With the availability of limited data, assessment of the magnitude of the disease burden in our country is underestimated.
There are many studies on clinical, epidemiologic, and virologic features of dengue in India which are focusedparticularly on tertiary health care hospitals, states and region24-31. There is lack of studies to assess the epidemiological and clinical features of dengue in the country. This study has attempted to understand the dengue infection in the population across different region over six years (2006-2011). In addition, we have assessed the clinical and laboratory features of patients hospitalized with dengue fever.
Materials and Methods
Study Settings
For this study, India was divided into five regions (south, north, west, east and central) to capture the diversity among different regions in the country. The incidence rates were obtained from national, regional or state surveillance systems and the official statistics of the Ministry of Health and Family Welfare based on which two states was selected from each region.Among which one state with a relatively high incidence rate of reported dengue cases and the second state with relatively low incidence rate of reported dengue cases.From each of these ten selected states, one medical college hospital was selected based on the availability of electronic medical data, willingness to participate, and ability to meet the study timeline and the quality requirement for this research. The sample of 10 medical college hospitals is designed to represent the range of dengue illness in each concerned state representing therespective region across India.The data was extracted from ten major hospitals in India, out of which two hospitals are pediatric hospital and remaining is general hospital.
Hospital based Retrospective Study Design
A retrospective cross sectional abstraction of dengue illness in hospitalized patients was carried out in 10 major medical college hospitals located in all five regions in India (Table 1 and Fig.1).For the retrospective component, the reference period for which data was extracted covering a period of six years starting from January 2006 through December 2011to achieve the study objectives of determining the clinical manifestation of dengue by severity across hospitals (study sites) and regions.
Criteria for selection of medical records (sampling) and data extraction tool
All the patients who were hospitalised during 1st January to 31st December of study years with a clinical diagnosis of Dengue/DHF/DSS (ICD10 code A90) were the sample frame. A systematic random sampling of 3000 medical records was planned to collect. The sample consists of 50 hospitalized patients in each of 10 medical colleges for six years. If there are 50 patients or fewer, we have included all those patients in the study. If there are more than 50 patients, a systematic random sampling was done to select 50 patients. All the selected medical records was carefully reviewed and classified according to the WHO criteria for diagnosis of Dengue, DHF and DSS. If the selected medical records were not available in the medical record department due to case sheet missing/patient absconded with case sheets, then the preference of selecting the medical record was given to consecutive record.
A data extraction instrument was developed to collect the required data from the medical records. The collection tool was focused on (1) socio-demographic details (2)data of admission and discharge (3) referral facility (4) admission and discharge diagnosis (5)patient's report of ambulatory visit/hospitalization prior to hospitalization at study sites (6) patient's report of date of onset of illness (7) setting (Casualty/ICU/Ward/Private room) (8) length of stay(nights) and total duration of illness through discharge (9) signs and symptoms (10)patient's temperature and blood pressure measurement at admission and discharge(11) dengue related laboratory investigation and other laboratory and imaging test (12) reclassification of dengue cases as per the WHO's classification.
See the REFERENCES for this paper here
Browse the Table that are used for Article here - PDF File
To be continued..
* Dr. Laishram Ranbir Singh (MD, FIAP, WHO Fellow) is a Professor and Head, Department of Pediatrics, at the Regional Institute of Medical Sciences (RIMS), Imphal Manipur.
He contributes to e-pao.net regularly and can be contacted at drranbirlai(aT)yahoo(doT)co(doT)in
This paper was webcasted at e-pao.net on 1st August 2015.
* Comments posted by users in this discussion thread and other parts of this site are opinions of the individuals posting them (whose user ID is displayed alongside) and not the views of e-pao.net. We strongly recommend that users exercise responsibility, sensitivity and caution over language while writing your opinions which will be seen and read by other users. Please read a complete Guideline on using comments on this website.


